The Uncinate Fasciculus neuroplasticity – How does it change with time and how does that change affect cognitive-emotional integration?
By Jenay Bartlett UA’25 (JB), Judah Weathers (JW), and Jim Stellar (JS)
Like any other brain structure, the Uncinate Fasciculus (UF) changes with age and with experience. This is called neuroplasticity. After our last blog on the UF’s basic function in cognitive-emotional integration, we return here to discuss these changes, particularly in a brain structure that can continue to develop in normal people through adolescence and into young adulthood, well past the typical college years. But first, what is neuroplasticity?
Neuroplasticity: The simple fact is that the brain changes its structure. It does so all the time in response to learning, to development, and of course to any damage. Every time you learn something, even at the smallest connections between neurons, there is change. As a father of modern neuroscience, Donald Hebb, once famously said, “Neurons that fire together, wire together.” These changes happen everywhere from the lowest and most early evolved neural circuits of reflexes in the spinal cord, to the most recently evolved and highest abstract processing in the prefrontal cortex. Much of modern neuroscience is devoted to understanding these changes in learning and in pathology like drug addiction, PTSD, Alzheimer’s disease, etc.
Neuroplasticity also occurs during normal development. One of the big early changes occurs in infancy underlying the development of complex skills and processing. For example, young babies do not have object permanence. When you hide behind something you are gone. They cannot really play peek-a-boo. But then, around 6 months or so of age, they seem to suddenly know that you still exist when you are hiding. Something connects in the brain that allows them to make this computation. There are many other examples of such changes in infancy and childhood over the years leading to more mature behavior as the hardware matures. Most of this is over by puberty, but the UF is one of the latest pathways in the brain to evolve and it is also one of the latest to fully anatomically mature, finally finishing by age 30.
That is really the topic of this blog. What gets finished in the development of the UF in the 20s? What are the implications, if any of this change for behavior, particularly in college students who take an internship to get some professional experience in their area of academic study? Given that the UF’s anatomy connects the prefrontal cortex to the amygdala and other areas, and given that this integration seems to affect cognitive-emotional integration, one has to wonder how much of this professional maturation in the 20s is due to development of the UF or to the experiences in that period that might lead to better executive control over emotions, such as fear. When a college student gains some maturity, like what happens when a premed student works in a hospital, how much of that change is from the experience itself and adaptations to the hospital setting and how much of that is simple anatomical wiring maturity in a pathway like the UF? Long ago, neuroscientists gave up trying to calculate the separate influences of environment and genetics and instead looked to how they might work together to produce change in neural circuits and behavior. However, one also has to wonder if America’s founding fathers knew what they were doing when they set the minimum age to be president of the USA to be 35?
Leaving Home: Neuroplasticity En Vivo
Try to think back to the first day living outside of the home you grew up in. Perhaps you grew up with a parent or caregiver that was convinced that you are not ready to live on your own yet. Alternatively, maybe they feel it was (high time) for you to leave home and take on your own responsibilities. Maybe it’s move-in day at college, or you have just become married and moved in with your partner. Any of these scenarios are likely to elicit a range of emotions in you: relief, anxiety, optimism, fear, hope, joy, regret; all of which are emotional states within which you must make important choices about how you will live, or not live, your life going forward. Interestingly, this major life transition typically occurs during the ages of 18’s to 30’s, a sensitive period of UF neuroplasticity connecting cognitive with emotional regions of the brain.
Let’s take this a step further. Growing up at home for a lot of people included having a parent that provided feedback (at times, neverending…) on what was ‘right’ or ‘wrong’ about your thinking or behavior. For those familiar with Sigmund Freud’s structural model of the human psyche, the parent therefore informs the development of our ‘super-ego’, imparting critical feedback on our developing thinking and behaviors, with the hope they will help us achieve our ‘ideal self.’ In the process, there is a great deal of cognitive-emotional integration that takes place, including how to perhaps make better choices to avoid painful, or achieve successful, outcomes.
Now, you have left home. You are a full-fledged adult, with all the skills you need to be happy and a successful member of society, right? Well, for those who answer ‘no’, do not be dismayed; cognitive emotional integration continues for several more years. Specifically as mentioned, the UF, which subserves communication between the prefrontal cortex (cognitive) and amygdala/limbic (emotion) regions, remains neuroplastic into and beyond 30 years of age. This neuroplasticity enables the UF to change in structure, and thereby support increasing cognitive-emotional integration based on learning, experiences, and time. This means the range of experiences we have as adults, from the dynamic relationships we have with the people we love or care about, to losses or adversity, all occur in the context of ongoing UF development and thereby impact cognitive-emotional integration.
Clinical Neuropsychology: Normative Development
During childhood, socioemotional experiences lay the foundation for UF development. As pruning and myelination occur, neuroscience typically observes the strengthening of white matter connectivity and reductions in gray matter, especially around 11-12 years of age. The gradual and extended fine-tuning of the UF may explain why we observe heightened emotional reactivity, impulsivity, and vulnerability to mood and anxiety symptoms during adolescence and young adulthood. During these years, we may not yet have the full ability to reflect on and regulate our emotions, as we are still in the process of learning how to integrate feeling and thinking.
Neuroimaging studies have shown increased strengthening of UF integrity over periods of development as measured in a brain scan called diffusion tensor imaging (DTI). DTI allows us to analyze fractional anisotropy (FA), which is a metric representing coherence and direction of a white matter tract. In the UF, higher FA is associated with people exhibiting improved emotional regulation and cognitive reappraisal – the ability to modify one’s emotional reactions in a given situation. This is because a more mature UF may support stronger top-down processing, allowing the prefrontal cortex to better regulate limbic emotional responses. Thus, we develop a stronger ability to reflect on everyday challenges–which we see as we mature as college students. For example, we learn to make decisions such as staying in and studying for an exam rather than going out to a social event.
While this learning and refinement of our cognitive-emotional integration continues throughout our 20’s we may still experience anxiety, stress, and burnout–all of which are completely normal. During this period, emotional regulation and self-reflection is demanded of us as we face things such as major life changes, academic stress, social comparison, and the pressure to pick the “right” path for ourselves. It may well be the job of the UF here to help us reframe stressful events, develop coping strategies, and make big decisions and long-term goals despite emotional challenges. As the UF continues to experience plasticity, it may become especially important during one’s time as college students that we continue to foster supportive relationships, seek mentorship, and surround ourselves with enriching experiences to support the development of our emotional wisdom and cognitive flexibility.
When we nurture the development of the UF, perhaps we are able to more effectively emotionally weigh our actions and decisions. We strengthen our own self identity as we make evaluations of what experiences felt right for us, and which may not be the most suitable. As we gain a clearer vision of our personal paths, we learn to differentiate between things such as an internship/job that may promote growth through manageable challenges and those that lead to emotional burnout.
Because our life experiences have such a strong influence on our neurodevelopmental process, the sensitive period of UF development also creates a period of heightened vulnerability. When we face adverse socio-emotional experiences, the typical development of the UF may be altered as well. In turn, this can affect cognitive-emotional processing, carrying possible clinical implications across behavioral, mental, and developmental areas.
Alterations in UF Neuroplasticity: Clinical Disorders
It comes as no surprise that, given the UF’s anatomical role in supporting communication between cognitive and emotional brain regions, problems that alter the neuroplasticity of UF can lead to disorders where cognitive-emotional integration is impaired. Indeed, research studies on UF development indicates the UF is still somewhat “immature” throughout adolescence and young adulthood, and this is an epoch where many pervasive clinical disorders emerge, including mood, anxiety, and post-traumatic stress (PTSD) disorders. The yet fully developed, neuroplastic UF is therefore vulnerable to alterations in its developmental trajectory in adolescence and young adulthood, including perhaps from genetic, social, stress, or environmental factors, that can result in disorders of cognitive-emotional integration.
Another way one can think of the UF in a medical reference is as the cognitive-emotional ‘epiphyseal plate of the brain’. The epiphyseal plates are the portions of long bones in the body that, during sensitive periods of bone growth and development, support the elongation of bones for gaining height and strength. Essential to the healthy function of the epiphyseal plate is proper nutrition, adequate exercise and rest, and avoiding damage (e.g. fractures or other injuries). Youth exposed to malnutrition or injury that involves the epiphyseal plate during this sensitive period of development are at higher risk of stunted growth or other bone abnormalities that will affect them for the rest of their life. While the UF is composed of different types of cells (e.g. glial cells) and growth factors (e.g. brain derived neurotrophic factor (BDNF)), it is a brain structure that, similar to epiphyseal plates in the bones, has a sensitive period of development that when disrupted can lead to lasting impairments.
DTI scans provide a means to study how the UF develops differently in clinical groups. For example, decreases in UF FA have been shown in adults with generalized social anxiety disorder. A recent meta-analysis of UF FA measures across approximately 23,441 adult individuals indicated decreased UF FA in depression, with comorbid anxiety moderating this effect in the left, but not right, UF. Bilateral UF FA was significantly decreased, in adults with generalized anxiety disorder, compared to healthy adults. Finally, in a group of military service members (average aged 29.5 years) that were exposed to combat, FA was inversely correlated with hyperarousal symptoms of PTSD.
In a DTI study of individuals with depression and a genetic variant of BDNF, a protein involved in neuroplasticity, DTI revealed decreased UF FA in individuals with the genetic variant compared to individuals without the genetic variant. A later study showed an interactive effect between the same BDNF genetic variant and childhood adversity on brain structure in depression. Further, there is growing evidence that the social experience, stress, and environment of developing youth also impact the UF structure. For example, youth with a higher neighborhood disadvantage score (i.e. composite score of educational attainment, poverty, housing burden, etc) had decreased right UF FA, a finding that was moderated by depressive symptom score. Taken together, there is increasing evidence that genetic, social, stress and environmental factors are deeply important in the healthy development of the UF and cognitive-emotional integration, and when healthy UF development is disturbed, clinical disorders can arise.
The Growing Age of Social Media and the Brain
There is growing scientific acceptance that brain white and grey matter development is likely to be influenced by social media use. Jonathan Haidt, a renowned social psychologist, has published extensively on the negative impact excessive smart-phone, social media, and high speed internet access has had on child and adolescent mental health. In his recent book The Anxious Generation, Haidt argues that recent exponential increases in rates of anxiety, depression, and suicide, emerging in ‘Gen Z’ members, is due to the introduction of “phone-based” learning and play, where the development of social, emotional, and executive functions happen primarily through virtual experiences instead of classic embodied (i.e. in person) and synchronous interactions with other humans. For example, phone-based social and emotional learning is riddled with false comparisons (e.g. ‘am I as attractive as these AI generated images’?) leading to negative self esteem, high “opportunity costs” (e.g. spending hours in a day scrolling through social media content, at the detriment of human-to-human, in person interactions where social and emotional skills are refined), and disruption to biologically ingrained cycles of wakefulness versus sleep (e.g. losing sleep thinking about how to get more ‘likes’, or doom scrolling), to name a few.
The asynchrony occurs in social media, for example, when children and adolescents are sending, receiving and processing emotionally salient information (e.g. ‘likes’, dislikes, self-comparisons, romance, etc) around-the-clock, instead of circumscribed times of person-to-person interactions. Ask any psychiatrist, low self-esteem, isolation from human-to-human interactions, and sleep-wake disturbances are core features of many mental health disorders now disproportionately effecting children and adolescents, including depression, anxiety and suicide. Furthermore, the ever present smart-phone, with its alerts, notifications, calls, and updates, can overwhelm that attention span of children and adolescents, including during school, at the dinner table, and while playing with friends. These types of sustained interruptions in attention and concentration are proposed to impair decision making and other executive functions. In sum, Jonathan Haidt argues the increasing rates of depression, anxiety, and suicide in developing children and adolescent are tied to the endless “disembodied”, asynchronous, and unrealistic social, emotional, and executive function learning they have on smart-phones.
Anatomical connections of the UF
According to one major 2021 study, the UF has five major subcomponents as listed below and as shown after the list in the figure below (which is figure 3 in their paper).
- dorso-lateral UF subcomponent connecting superior-medial-inferior frontal cortex to the superior-middle-inferior temporal pole,
- ventro-lateral UF subcomponent connecting orbito-frontal cortex regions to the middle and inferior temporal pole,
- ventro-medial UF subcomponent connecting medial orbito-fronto cortex to the temporal pole,
- short postero-medial UF subcomponent connecting the posterior part of the orbito-frontal and rectus gyri with the temporal pole and fusiform gyrus,
- short antero-medial UF subcomponent connecting orbito-frontal and rectus gyri with the most antero-medial part of the STG and ITG temporal gyri,
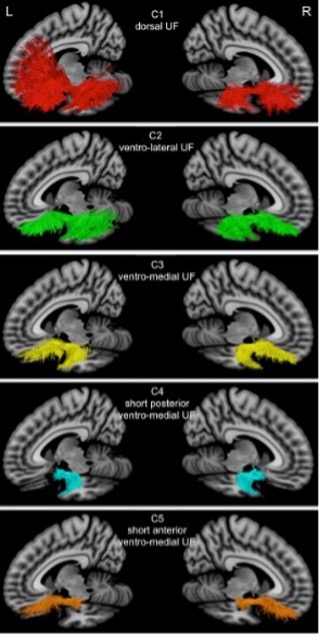
We show this figure and the list above to illustrate the complexity of this pathway. To go through the details is beyond the scope of this blog, but in each pathway (and perhaps subpathways) there is the opportunity for neuroplasticity associated with UF development that could alter functioning.
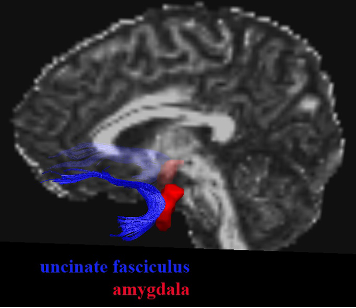
Given our past blog on the UF-amygdala connections and anxiety, we also looked at a 2012 study that specifically examined the UF-amygdala connections as shown in the figure below. In their report, the volume of the left hemisphere amygdala and UF were particularly related to anxiety, but not so significantly in the right hemisphere. Left-right hemisphere distinctions are noted here but again are beyond the scope of this blog.
Are we “stuck” after the UF is developed?
Although we mention that the UF reaches full development around one’s thirties, this doesn’t mean that neuroplasticity stops here. “Development” in this context is used to mean that the UF exhibits structural maturation–white matter volume, organization, and myelination are optimized for peak efficiency–and this optimized functioning may be more difficult to change. However, despite the structural formation of the UF being less malleable, neuroplasticity can still occur.
In fact, through principles of learning, we can make active efforts to improve our emotional regulation and cognitive input. Of course, our early development and experiences serve as a strong blueprint to our cognitive-emotional behaviors, but these habits do have the ability to be reshaped. For example, a 2011 study showed that cognitive-behavioral therapy (CBT) was associated with stronger structural integrity of the UF in patients with autism. Similarly, a 2013 study on patients with Obsessive Compulsive Disorder (OCD) showed improvements in white matter structure in midbrain regions following CBT. CBT in particular draws on principles of classical and operant conditioning, using reinforcement to modify maladaptive behaviors. Specifically, techniques such as cognitive reappraisal or exposure response prevention utilize these principles of learning to retrain our neural pathways for improved communication and healthier functioning. These studies show that our brain is not fixed, and some functioning can actively be changed based on our choices, experiences, and actions. It is this ability that we should remember as we proceed in our lives, taking it as both reassurance and a responsibility that even in adulthood we continue to actively shape the emotional and cognitive paths our brain follows.
A follow-up will be a next blog on the continued development of the UF and what it means for college-age students and people in general who are coping with challenges, like a PTSD-inducing experience.